
Safe surgery on thyroid gland
This website aims to provide you with complete and valid information about thyroid surgery. I am a certified endocrine surgeon. I have been trained by Prof. G. Kapelakis at the Eugenides Hospital. I am a regular member of the Hellenic Society of Endocrine Surgery, the American College of Surgeons and BAETS (British Association of Endocrine and Thyroid Surgeons). I am very proud to update my website so that you can be fully informed about the progress in thyroid surgery.
Thyroid surgery can theoretically be done by all general surgeons. However, it is a demanding surgery and when performed by a specialized surgeon, it has minimal chances of complications. The size of the incision is very important since one will have it for the rest of one’s life and even in a prominent place. It is a demanding surgery because the thyroid comes in contact with the nerve that is responsible for speech and the parathyroid glands. It takes expertise and extensive experience to remove the entire gland without injuring the nerve.
Minimally invasive thyroidectomy
The operation I perform is called “minimally invasive total thyroidectomy”. This operation reduces your stay in the hospital to one day, as there is no pain at all.
Section size
The incision in the skin is minimal which is difficult to distinguish after a few months and does not require cutting of the neck muscles. Some cases are not suitable for mini surgery, but even in these the incision in the skin is very small. Some studies show that only 10% of patients are eligible for “minimally invasive thyroidectomy”. But this is not my opinion either. In my experience more than 60% of my patients can benefit from this method. Nodules larger than 3cm or thyroid tumors are not in themselves, for me, an obstacle to performing this operation.
Thyroid residue
The residue I leave in 90% of my patients is less than 1% while in the rest it is not more than 1.8%. The importance of the residue is great. In cases of cancer, it depends on how many sessions of radioactive iodine a patient will have. Also, if reoperation is needed to remove the remaining gland. Reoperation, however, has higher rates of complications and great suffering for a patient, both mental and physical as well as financial. However, with the total thyroidectomy that we perform, such cases do not exist in us.
Hospital Stay
The fact that you stay in the hospital for a day has to do with your safety. Immediately after the operation you talk and after a few hours you walk and eat. Impression is not my priority but the safety of the man who trusts his life in my hands.
Possibility of complication
All surgeries potentially have a complication rate, in all surgeons, worldwide. Going out on the same day does not offer anything significant, in my opinion and in my experience. I never give calcium to my patients postoperatively, unless needed and this is extremely rare. Checking and confirming the price of calcium the next day, with a blood test is imperative, this is the main reason for your stay. I do not agree with his tactic of giving all patients postoperative calcium to cover a hypoparathyroidism and the patient leaves the same day.

Thyroid Gland Surgery – Internet Medicine
The internet is full of medical advice. A team of Australian surgeons reported the fact that there is incorrect or false information at a frequency of 30%. This highlights how important it is for you patients to always seek professional advice. The widespread perception of internet medicine is not a substitute for direct and “face to face” examination and information by the doctor.
You should not be ashamed or embarrassed, but ask your doctor about anything that concerns you. You need to be aware of the possible complications and risks of surgery. Research has shown that a surgeon’s experience plays a major role in a safe and successful thyroid surgery.
Most surgeons welcome your questions, knowing that we do not exist for our benefit, but for your own good. We consider it our privilege to deal with these diseases. An experienced surgeon does not exaggerate his experience and success, nor does he insultingly refer to other surgeons or doctors.
IMPORTANT
Thyroid gland surgery – Thyroidectomy

Thyroidectomy is the surgical removal of part or all of the thyroid gland. Lopectomy is the surgical removal of a single thyroid gland. Thyroidectomy is recommended for patients with goiter, thyroid nodules, hyperthyroidism, or thyroid cancer. Total thyroidectomy is a very good choice for patients who have large goiter, nodules or thyroid cancer.
Thyroid surgeon Stavros Tsirigotakis performs safe and effective thyroid surgery. During thyroid surgery, the laryngeal nerves and parathyroid glands must be protected and maintained. This is ensured by his knowledge and experience, but also by the technological equipment he uses when needed (neurostimulator to locate the nerve, ultrasound scissors, etc.). His experience and practical experience, which is more than 18 years in this surgery, guarantees that the possibility of complications is minimal. Drain pipe is not usually used for these operations.
Neurostimulator – monitoring of the nerve during surgery, with state-of-the-art technology

Special oxygen delivery tube, when a neurostimulator is used
The evolution of technology offers us state-of-the-art equipment, which we use for safer interventions. Nerve monitoring is performed in thyroid surgeries where the anatomical position of the nerve is complex or has changed after previous neck surgery. A special endotracheal tube (anesthesia tube for oxygen delivery) with an electrode is used (picture below). It is connected to a special device that produces visual and audible signals when manipulating the nerve area and this helps to locate it in difficult cases (picture below).
Thyroidectomy in thyroid cancer
It is very important that the initial operation is as perfect and complete as possible, because your prognosis depends on it. This means that if the operation is “incomplete” surgery (and unfortunately this is not uncommon):
- the ability to control the disease is impaired
- is likely to cause the need for additional surgery
- the chances of complications during reoperation increase
- potentially undermines survival.
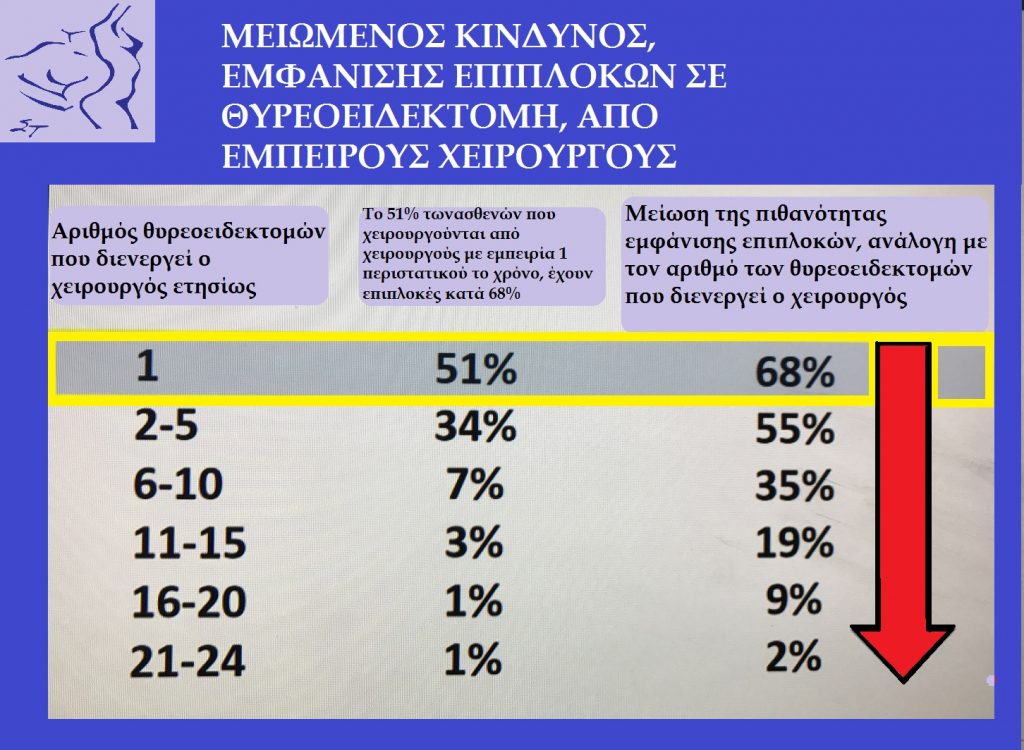
The volume of patients that a surgeon operates annually is a criterion for patient safety

A specialized thyroid surgeon is a prerequisite for safe surgery
Minimally Invasive Thyroidectomy Assisted Camcorder (Minimally Invasive Video Assisted Thyroidectomy MIVAT)
The Minimally Invasive Thyroidectomy Assisted Video (MIVAT) or endoscopic thyroidectomy carried out using a high-resolution camera in surgery through a very small incision. It is an excellent choice for patients with thyroid cancer or nodules, with dimensions less than 3cm. This technique allows thyroidectomy to be performed through smaller incisions. It is safe and effective, as it offers faster recovery and less inconvenience to patients.
Thyroid Gland Surgery – Minimally Invasive Thyroidectomy
In thyroid surgery gland, minimally invasive thyroidectomy is thyroid surgery performed through an incision that is 3cm or less. Patients usually have less pain faster recovery, compared to traditional traditional thyroidectomies and certainly minimal scarring. The size of the scar is very important, since the postoperative scar is in a visible place and the patient will have it for life.
Surgical thyroid gland – Thyroid reoperation in
Reoperations are performed in patients with recurrent thyroid cancer or in patients who underwent surgery for Graves’ disease and the disease recurred due to defective surgery. It is also performed on patients who, while undergoing surgery for cancer, have a large residue left. The previous surgery increases the risks of the second thyroid surgery. Reoperation is always more difficult. These surgeries are best performed by surgeons such as Stavros Tsirigotakis with specialized training and many years of experience.
Lymph node dissection in thyroid cancer

Cervical lymph nodes that can be infiltrated by thyroid cancer
In thyroid surgery, when the presence of thyroid malignancy has been diagnosed, then the operation to be performed is oncological surgery. There is a difference between a surgery performed for a benign condition and a malignant one. For malignant disease the operation is oncological surgery. The oncological operation, among others, lies in the removal of the lymph nodes along with the removal of the organ that has the cancer. When there is thyroid cancer, it can sometimes affect the lymph nodes in the throat. Even depending on the type of cancer we know that it will affect them later with certainty.
Lymph nodes
Therefore it is necessary in these cases to remove the lymph nodes from the throat. There are many lymph nodes in the neck. They are located below or around the thyroid gland, trachea, esophagus, carotid artery or even some distance from the thyroid gland. We need to know if they are infiltrated before the operation. During the operation we must remove them, with the aim and goal of preventing the cancer from spreading.
Identifying and locating them helps us a lot in this. This is done through high definition ultrasound. Their mapping and the cytological examination we receive through puncture (FNA) are very important. Mapping determines the plan of surgery, which is the main treatment for thyroid cancer. The life of our patient depends on the quality of thyroidectomy.

Cervical mapping in thyroid cancer is necessary
The body’s lymph nodes are organs that can be compared to the carbon filter system. This way the cancer cells can be trapped inside the filter. The body does not have any means to eliminate the cells it has captured, they are constantly stuck there and begin to grow inside the lymph node.
There are two types of lymph node dissection for thyroid cancer:

Lymph nodes must be removed when they are infiltrated by cancer
Thyroid surgery – Central Lymphatic Cleansing
In thyroid surgery, when there is thyroid cancer and the lymph nodes are infiltrated by cancer, lymph node dissection is required. This involves removing the lymph nodes located near the thyroid gland. Stavros Tsirigotakis performs this surgery always when needed for the patient diagnosed with thyroid cancer. It is the removal of lymph nodes in the area of the larynx and trachea. This area extends from the trachea to the carotid artery. It reaches down to the upper part of the thoracic cavity. This surgery is called level VI lymph node dissection.
ENDOCRINOLOGICAL SURGERY IS OUR PASSION
Thyroid surgery – Lateral Lymphatic Cleansing
In thyroid surgery, lateral lymph node dissection is the removal of lymph nodes on the sides of the neck. The cervical lymph nodes are divided into levels and numbered in Latin numerals (levels I-VI). This surgery is the removal of the lymph nodes from levels II, III, IV and V.
In these areas there are many nerves and large blood vessels that are at risk for injury during these types of surgeries. This type of surgery is only recommended if thyroid cancer has been shown to have infiltrated these lymph nodes.
Types of thyroidectomy depending on the disease
Demanding surgery
As with any surgery, there is a risk of complications in lateral lymph node dissection, which is performed in thyroid surgery. In the hands of an experienced surgeon, this risk is low. Endangered nerves include the retrograde laryngeal nerve, the phrenic nerve, the spinal cord, and the cervical nerves. The retrograde laryngeal nerve innervates the vocal cords and an injury can affect the voice. The phrenic nerve controls breathing, innervates the diaphragm, and an injury can cause respiratory problems. The spinal nerve controls the movement of the shoulder, its injury can cause weakness in the shoulder.
The large blood vessels in the area are also at risk and include the carotid artery and the internal jugular vein. The thoracic cavity is also at risk during this type of surgery and an injury to it may require drainage.

In thyroid surgery, in order for the operation to be safe, one way is to leave part of the thyroid gland where the nerves and the parathyroid glands are located so that the surgeon does not reach them and injure them. This is an almost total thyroidectomy. “Based on my experience, I avoid this operation. Because if the histological examination shows cancer, patients are very likely to need repeated sessions with radioactive iodine or even reoperation. Also if the patient has Graves’ disease, it is possible with almost total thyroidectomy, recur after surgery and need reoperation. “Reoperations bother the patient and have an increased incidence of complications.”
THYROID SURGERY – MINIMUM INVASIVE THYROIDECTOMY
In thyroid surgery, the operation performed by thyroid surgeon Stavros Tsirigotakis is usually the minimally invasive ampho total thyroidectomy. That is, through a very small incision, it removes the entire thyroid gland, without cutting the neck muscles. This is because the experience of surgeon Stavros Tsirigotakis has shown that several times the patient is operated on for a suspicious nodule that is not cancer and there is cancer in the other lobe. Or is operated on for goodwill and the histology after the surgery shows that at some point cancer had developed and this is not uncommon.

Very small incision in minimally invasive thyroidectomy
A single operation is enough
It is best to operate on the patient, most of the time, as if the malignancy is confirmed. So if malignancy is diagnosed, the residue should be almost zero so that neither many iodine sessions nor reoperation are needed. Ensuring the integrity of the nerves and parathyroid glands lies on the one hand in the experience of surgeon Stavros Tsirigotakis. And on the other hand in the state-of-the-art technological equipment it uses. It does this to provide patients with the best and safest results.
Minimally invasive thyroid removal
Thyroid surgeon Stavros Tsirigotakis performs minimally invasive thyroidectomy. That is, through an incision of 2-3 cm, which is the smallest possible, it removes the entire thyroid gland, without cutting the muscles. The size of the incision is important not only for the aesthetic result, but also shows the surgeon’s familiarity with the specific operation.
It is well known that the less injuries and injuries are done in an operation the better the result. Of course, it is easy to imagine what kind of injuries would have occurred during an operation that leaves a huge postoperative scar. If it is deformed, the patient will be obliged to have it for life at a clear point in his neck.
Fixation scintigraphy
Confirmation of removal of the entire thyroid gland is demonstrated by examination. This test is called a scintigraphy or fixation test, which is done after surgery, when the histology shows that it is cancer.

In minimally invasive thyroidectomy, the incision is minimal, covered by the thumb
So that shows with unprecedented accuracy rate of thyroid remaining after this will then be destroyed by administration of radioactive iodine. If it is up to 2% it is accepted by the scientific community (it is worth noting that the human eye of the surgeon can distinguish from 1% and up).
Our results
In approximately 95% of the cases of the patients operated by the surgeon Stavros Tsirigotakis, the thyroid residue is less than 1%. So it is obvious what treatment his patients will receive compared to the treatment given by someone who has a residue of 4% or 8% or even 10%. Patients with large residues need reoperation. However, it has much higher rates of complications, in addition to the additional mental, physical and financial suffering of the patient.

The best result is the almost zero residue in thyroid surgery for malignancy
Optimal result
For this reason, Mr. Tsirigotakis seeks and has special care to ensure the best result for patients with a single operation. It is performed through an incision that after a while is difficult to distinguish. Below are some opinions from this examination. It has been done by patients of Mr. Tsirigotakis, to diagnose how much thyroid residue is left. In fact, he did not operate on these patients for thyroid cancer but for goodwill. However, the histological examination after the surgery showed that it was cancer.
It is easy to see why patients who have been diagnosed with cancer preoperatively are not included. In these patients, it is imperative and planned from the beginning to remove the entire gland, at the time of surgery for cancer. Here by default the residue must be almost zero.
Residue
Therefore, one can imagine what will be the thyroid residue that a patient will have, who will be operated on for thyroid cancer by the surgeon Stavros Tsirigotakis. In these cases the concern to remove the last thyroid cell is very high. The residue left on thyroidectomies for benign is less than 1%.
Regulation
It is easy to see how easily a patient can be adjusted with medication postoperatively even when he has undergone benign surgery with a residue of less than 1%. On the contrary, it is understandable how difficult it can be to regulate when a large part of the gland has not been removed. The endocrinologist then tries to regulate it by giving him medication but at the same time the residue that has also produced hormones. So he is forced to constantly change the dose by doing repeated blood tests.